Non-Surgical Treatment for Women Suffering from Accidental Bowel Leakage
Do you suffer from Accidental Bowel Leakage?
Is Accidental Bowel Leakage (ABL) taking over your life? Are you unable to do the things you want because of bowel control issues?
If you answer yes to any of the following questions, this could be the case:
Do you sometimes have bowel movements too frequently?
Do you sometimes have difficulty completely emptying your bowels?
Do you ever notice staining/soiling/leakage?
Do you sometimes experience a strong urgency to have bowel movements?
Do you ever have “close calls? (i.e. rush to the bathroom)?
In general, are you ever unsatisfied with your bowel control?
Are you interested in improving your bowel control?
You don’t have to let Accidental Bowel Leakage disrupt your life. The Eclipse™ System for Bowel Control provides women with a low-risk, non-surgical solution to help prevent accidental stool loss.
Learn more about Accidental Bowel Leakage from Dr. Holly Richter:
Accidental Bowel Leakage (ABL), also called Fecal or Bowel Incontinence, affects over 10 million women1 in the U.S. It typically starts between ages 47 and 553 but can start as early as the 20s2. ABL becomes more common in women as they reach their 50s, 60s, and 70s2. It can greatly impact quality of life, leading to social isolation and a higher need for long-term care4. The financial costs can also be high, with average yearly medical expenses around $2,4005. If surgery for a neuromodulation implant is needed, the cost can go up to about $36,0006.
Why do women experience Accidental Bowel Leakage (Fecal Incontinence)?
Fecal Incontinence can be caused by many factors, such as birth defects, nerve issues, muscle damage, or pelvic injuries3. For example, the muscles supporting the bladder, rectum, and uterus can weaken or get damaged due to pregnancy, childbirth, pelvic injury, aging, and other reasons. Further, having one pelvic floor disorder is linked to a higher risk of having others. In a study, 57% of women with Urinary Incontinence also had Fecal Incontinence or Accidental Bowel Leakage7
People with Accidental Bowel Leakage may experience:
Urgency: A sudden, strong need to have a bowel movement
Passive soiling: Passing stool without realizing it
Incomplete emptying: Stool remaining in the rectum can leak out later
Frequent bathroom trips: Feeling the need to go often
Staining: Stool stains in underwear
Living with Accidental Bowel Leakage may involve:
Fear of accidents and unpleasant odors
Social embarrassment, shame, and avoiding social activities
Limited mobility and planning life around bathroom access
Financial strain, possibly being unable to work or work as usual
Challenges with intimacy
Reduced physical activity, leading to weight gain or other health issues
Disrupted sleep due to bathroom needs
Fewer wardrobe choices
Difficulty traveling, needing to pack extra clothes, sheets, and bags
Feelings of isolation and depression
Skin irritation
Accidental Bowel Leakage is Underreported and Undertreated
Alarmingly, most women with Accidental Bowel Leakage do not seek care. In a study, approximately 70%8 of women with Accidental Bowel Leakage chose not to discuss the condition with their physicians.
Reasons for not speaking up may include the following:
Embarrassment
Belief that it’s a normal part of aging
Lack of awareness about treatment options
Developing ways to cope with it
Other
Treatment Options for Accidental Bowel Leakage
Treating Accidental Bowel Leakage is not just about managing the symptoms, but also about helping women regain their independence and confidence to live without anxiety or embarrassment. Unfortunately, there have been few effective treatments for bowel control issues.
Initial treatments for Accidental Bowel Leakage may involve various lifestyle changes like adjusting your diet, using fiber supplements, and wearing diapers or pads.
Conservative medical options may include pelvic floor physical therapy and medications.
More advanced treatments may include injecting bulking agents into the rectum, surgery to implant a neuromodulation device, repairing the anal sphincter, and diverting the colon with an ostomy, where a bag collects stool.
Eclipse System for Bowel Control
The Eclipse System is a newer, FDA cleared, and non-surgical option for treating Accidental Bowel Leakage in women. It works as well as surgically implanted nerve stimulation devices3 like Axonics or InterStim. Eclipse is available by prescription and can be conveniently fit in a doctor’s office. It’s designed for adult women with Accidental Bowel Leakage and can be used alone or with other treatments to improve bowel control.
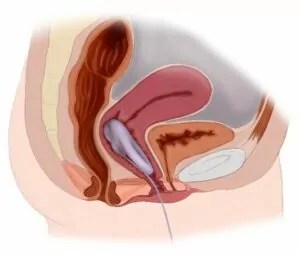
Eclipse is a removable vaginal insert with a small balloon that gently presses on the rectum to stop stool from passing. Placed in the same location as a tampon, the patient inflates the insert’s balloon to prevent stool from passing using a separate small pump. When it’s time for a bowel movement, the patient deflates the balloon with the same pump, allowing stool to pass normally. Afterward, the balloon is reinflated to block stool again. The separate pump is compact and can be easily stored in a handbag.
UNINFLATED DEVICE for bowel movement INFLATED DEVICE to prevent stool leakage
Accidental Bowel Leakage may be treated by different types of doctors depending on the cause. Here are the specialists who may help:
Urogynecologists (Urogyns): These doctors specialize in treating Pelvic Floor Disorders in women, including Urinary and Fecal Incontinence. They are experts in fitting devices like pessaries, which is similar to fitting the Eclipse Insert. Urogyns are the most likely physician to treat Accidental Bowel Leakage with the Eclipse System.
OB/GYNs: These doctors focus on pregnancy and female reproductive health. Some may treat Accidental Bowel Leakage, such as postpartum cases, or refer patients to a Urogyn or other specialist depending on the cause.
Colorectal Surgeons: These surgeons treat diseases of the intestines, colon, rectum, and anus. While they handle complex cases requiring surgery, they may refer patients without a surgical need to other specialists.
Gastroenterologists (GIs): These doctors focus on digestive system health and perform procedures like colonoscopies to diagnose issues. They treat conditions such as pancreatic disease, irritable bowel syndrome (IBS), GI cancers, and acid reflux.
Will Eclipse work for me?
If you are a woman with Fecal Incontinence and have no vaginal infections or open wounds, you may be a candidate for Eclipse. In the LIBERATE study, 62% of women were successfully fit4. Since Eclipse is a non-invasive option, it can be tried before considering more invasive treatments like surgery. Eclipse is easily removable, making the therapy low risk and reversible.
Getting fit for Eclipse is done conveniently from your doctor’s office. First, your healthcare provider will check your vaginal health to make sure you’re ready for Eclipse. In some cases, they might prescribe an estrogen cream beforehand to improve tissue health.
Once you’re ready, your doctor will use sizing rings (similar to those used for a pessary) to find the right size insert for you. Then, a temporary, disposable Eclipse Trial Insert will be used to confirm the overall insert fit. Different sizes can be tried to ensure it’s comfortable and effective for your body.
Your doctor may let you use the Trial Insert at home for up to two weeks to see how it fits, how comfortable it is, and how well it works for you. If the trial is successful, you’ll receive your long-term Eclipse Insert, which lasts for 12 months. After a year, you’ll return to the doctor for a replacement.
Eclipse Effectiveness
The Eclipse system has been tested in over 200 women10.
In the LIFE study3, 86% of women reported treatment success* after 1 month of use. The average number of Fecal Incontinence episodes dropped from 5.8 per week before Eclipse to 1.1 per week after Eclipse at 1 month with 41% of participants having no accidents. Eclipse not only reduced accidents but also improved bowel control symptoms. These symptom improvements included less urgency, less incomplete bowel movements, less frequent bowel movements, and less liquid stool3.
In the longer-term LIBERATE study4, 84% of women reported success* at 3 months, and 94% of those who continued in the study reported success at 12 months. The number of Fecal Incontinence episodes went from 7.1 per week before Eclipse to 1.5 per week at 3 months, 1.1 per week at 6 months, and 0.9 per week at 12 months after Eclipse4. At the end of the 12-month study, 46% of women reported no Fecal Incontinence episodes4.
The fit rate for Eclipse during the LIBERATE study was 62%4, meaning it won’t work for everyone. However, because Eclipse is non-surgical and can be tried in a doctor’s office before committing, it’s easy to see if it works for you. In the LIFE study, 96% of women found Eclipse “comfortable or could not be felt”, and 98% said they would recommend it to a friend3.
Eclipse Safety
Eclipse has been proven to be safe and low risk in several clinical studies, including the LIFE3 and LIBERATE4 studies. No serious device-related adverse events were reported. However, some women did experience mild adverse events**. In the LIFE study, the most common issue was “pelvic cramping or discomfort”, mostly during the fitting period3. The next most common issues were urinary incontinence “or urinary urgency or frequency”. In the LIBERATE study4, the “most common adverse event was vaginal wall injury, with most adverse events occurring during fitting period.” None of these events caused women to leave the LIBERATE study.
Summary
Eclipse is a low-risk, non-surgical, and highly effective solution for Accidental Bowel Leakage. With just a simple visit to your doctor’s office, you could regain bowel control. Unlike surgically implanted devices, Eclipse is easily placed and removed, so you can use it as needed. It can also be combined with other bowel control treatments to give you more confidence in your daily life.
Talk to your doctor today to see if Eclipse is right for you.
Do you need help finding a physician to treat your Accidental Bowel Leakage? Try our Find A Provider tool or contact us directly via Laborie Contact Form.
For more information from physicians and patients, explore our interactive Eclipse experience below
Eclipse Questions and Answers for Patients
The inability to control your bowels which results in the leakage of stool – also known as Fecal Incontinence (FI) or a loss of bowel control or bowel incontinence.
The cause of Accidental Bowel Leakage can have several origins including nerve or muscle damage in the pelvic region which can affect bowel control, as can diarrhea, Irritable Bowel Syndrome (IBS) or other gastrointestinal conditions. Prior childbirth is also associated with Accidental Bowel Leakage.
Eclipse is a vaginal insert, placed in the same location as a tampon. The Insert has a balloon on it, which can be inflated to prevent stool from passing. A small, detachable pump is used to inflate and deflate the balloon. When you’re ready to have a bowel movement, you simply deflate the balloon. There is no need to remove the insert. Once you have finished your bowel movement, inflate the balloon again and go on your way.
The Eclipse System is indicated for the treatment of fecal incontinence in adult women. It is intended for prescription use. It should not be placed while there is a current vaginal infection or open vaginal wound.
Eclipse was cleared by the FDA in 2015 and is prescribed by physicians with knowledge in the evaluation of pelvic floor anatomy. Thus, Eclipse is currently not available OTC.
Diagnosis: The patient visits a doctor who prescribes Eclipse. The doctor reviews your health history and performs a pelvic exam to ensure you’re a good candidate. If needed, a topical estrogen cream may be prescribed to improve vaginal tissue before fitting Eclipse.
Sizer and Trial Insert Fitting: During the same or a future visit, the doctor may try different Sizers and temporary Trial Inserts to find the right fit for you.
Eclipse Fitting: If the Trial Insert is comfortable, you’ll be given the Eclipse Insert, which lasts for one year, to take home and use.
Follow-up: It may take a few days to get used to using Eclipse, and patients are encouraged to contact their clinic with any questions or concerns.
The Eclipse System (insert and pump) should be replaced yearly by your healthcare provider.
Many women who use Eclipse are sexually active. You should remove the insert prior to vaginal intercourse.
No studies have been conducted of women who use a tampon while wearing Eclipse. You should remove any tampons or other vaginal inserts prior to inserting Eclipse.
Your physician will need to see you to assess whether Eclipse will be a good option for you.
You cannot use Eclipse and a pessary at the same time. In addition, the Eclipse system is not intended to replace your pessary. Your physician will need to see you to evaluate what’s most appropriate for your body and overall treatment needs.
There are detailed cleaning instructions in the Eclipse System User Guide. You can use soap and water to clean your insert. You should remove the insert to clean it at least once a week or daily if worn during menstruation.
Eclipse contains metal and so must be removed before undergoing an MRI, in order to prevent any potential adverse events that may occur due to heating or movement of the Insert during the MRI. Eclipse is designed to be removed by patient when needed including for medical procedures or for periodic cleaning.
The safety and effectiveness of the Eclipse System have not been evaluated in patients with pelvic organ prolapse beyond the plane of the hymen or who are pregnant. Stage 1 or 2 prolapse will typically be OK with Stage 3 being more difficult to successfully fit.
The use of the Eclipse System after a recent hysterectomy may compromise the integrity of the vaginal cuff repair.
Eclipse has Medicare coverage under HCPCS Code A4563. The patient responsibility will vary depending upon your type of coverage including supplemental insurance. Private Pay insurance coverage will vary. Your physician’s office can help work with your insurance provider to determine eligibility and coverage amounts including getting a prior authorization.
Learn more about using Eclipse from Meghann Scott, RN:
Nygaard et al. Prevalence of Symptomatic Pelvic Floor Disorders in U.S. Women. JAMA 2008; 300(11):1311-1316.
Bharucha AE et al. Prevalence and Burden of Fecal Incontinence: A Population-Based Study in Women. Gastroenterology 2005;129:42–49
Richter HE, Matthews CA, Muir T, et al. A Vaginal Bowel-Control System for the Treatment of Fecal Incontinence. Obstetrics & Gynecology 2015; 125(3):540-547
Richter HE, Dunivan G, Brown H, et al. A 12-Month Clinical Durability of Effectiveness and Safety Evaluation of a Vaginal Bowel Control System for the Nonsurgical Treatment of Fecal Incontinence. Female Pelvic Med Reconstr Surg. 2019; 25:113-119
Xu X et al. Economic Cost of Fecal Incontinence. Dis Colon Rectum 2012; 55: 586–598
Bernstein et al. Three-Year Cost-effectiveness […] Management of Fecal Incontinence. Clinical Therapeutics. 2014; 36(6):890–905
Lawrence et al. Prevalence and co-occurrence of pelvic floor disorders in community-dwelling women. Am College of Obstet Gynecol 2008; 111(3):678-685
Brown et al. Factors associated with care seeking women with accidental bowel leakage. Female Pelvic Med Reconstruct Surg. 2013; 19: 66-71
ACOG Practice Bulletin #210, April 2019
Eclipse Instructions for Use – ART-0459 Rev.01
Study definitions:
*Study success criteria defined as at least a 50% reduction in fecal incontinence episodes in the post-Eclipse period versus the pre-Eclipse period.3,4
**Adverse event definitions:
The LIFE Study defined adverse events “as any untoward medical occurrence, unintended disease or injury, or untoward clinical signs (including abnormal laboratory findings) in consented participants, whether or not related to the investigational medical device, were documented.”3
The LIBERATE Study defined adverse events “as any untoward medical occurrence, unintended disease or injury, or untoward clinical signs (including abnormal laboratory findings), were documented, and relationship to the investigational device was assessed.”4



 Accidental Bowel Leakage is Underreported and Undertreated
Accidental Bowel Leakage is Underreported and Undertreated Eclipse System for Bowel Control
Eclipse System for Bowel Control